Exam 1 PD Objectives
From Iusmicm
[edit] Chapter 19: Female Genitalia
- Pages 549-583.
- Identify and describe the components of the physical examination of the female genitalia.
- Too long. See outline given at SPD.
- Recognize abnormalities that can be found on each component of the exam.
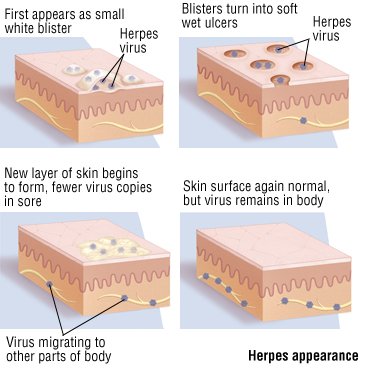
- Recognize and differentiate the clinical features of genital ulcerations.
- The three primary genital ulcerations are: herpes (HHV), syphilis (T. pallidum), and chancroid (Haemophilus ducreyi).
- Distict features of sphyilis: long incubation time (9-90 days), a single ulcer, painless, rarely recurrent.
- Distict features of herpes: vesicular, heals within 2 weeks
- Distict features of chancroids: multiple papules / pustules.

- Painful (herpes, chancroid) -> vesicle (herpes), papule / pustule (chancroid)
- Painless (syphilis)
- Multiple ulcers (herpes, chancroid) -> (

- Describe and give recommendations for screening for cervical cancer for a patient based on the American cancer Society recommendations.
- Beginning at 21yo, screen with Pap smear (or every 2 years with liquid-based prep).
- Beginning at 30yo (with three normal, consecutive paps and no complicating factors like hx of STIs), screen with Pap smear every 2 or 3 years. One can also screen in these conditions every 3 years (but not more frequently) with the HPV DNA probe.
- Beginning at 70yo (with no abnormal paps in the last 10 years and no complicating factors like recent hx of STI), one can discontinue screening.
- Define and recognize the following sequelae of pelvic floor relaxation: cystocele, rectocele, and uterine descent.

- Define and differentiate the following: amenorrhea, menorrhagia, metorrhagia, menometrorrhagia, and postmenopausal bleeding.
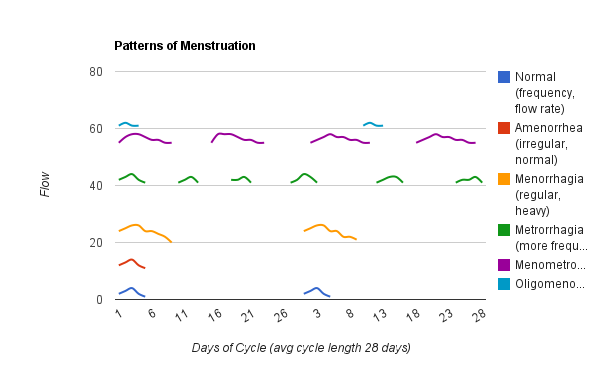
- Post-menopausal bleeding occurs...after menopause.
[edit] Chapters 13 & 14: The Chest and the Cardiac Examinations
- Pages 362-390, Pages 391-437
[edit] Chapter 13
- Describe the topographical landmarks of the chest and utilize that knowledge to describe physical findings of the chest.
- Recognize the main symptoms of pulmonary disease and how these symptoms can identify disease.
- Interpret the symptoms of pulmonary disease and apply them clinically to a patient.
- Apply the components of the physical exam of the chest to a patient.
- Clinically correlate the symptoms and physical exam findings pertaining to the chest:
- Pulmonary Edema
- Pneumothorax
- Asthma
- Pneumonia
- Emphysema
- Pulmonary Embolism
- Pleural Effusion
- Generate a diagnosis and/or differential diagnosis based on symptoms and/or physical exam findings of the chest.
[edit] Chapter 14
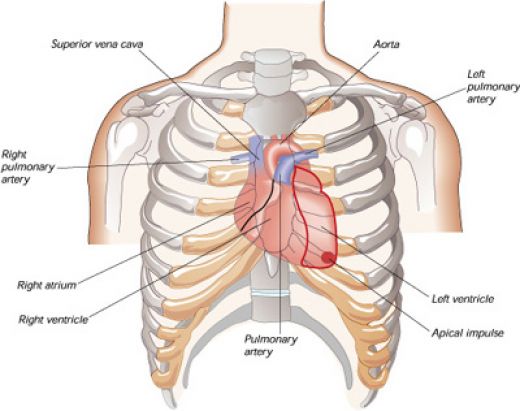
[edit] Describe and recognize the surface topography of the heart and utilize that knowledge to describe the physical findings of the heart

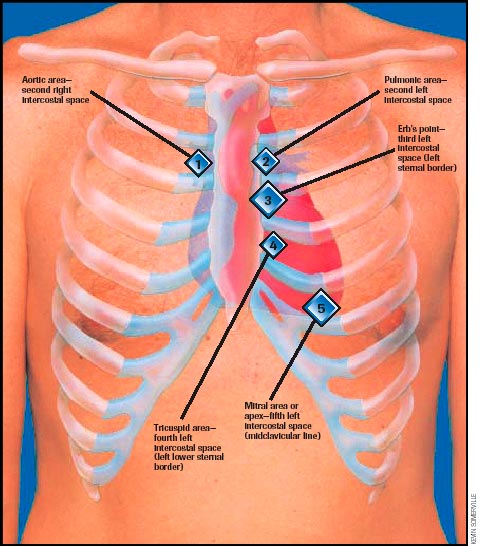
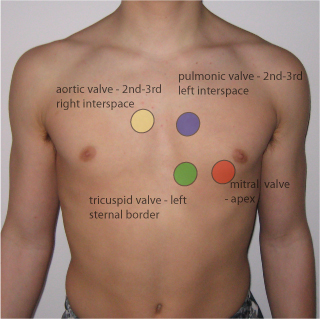
[edit] Describe and recognize the four classic auscultatory areas and Erb’s point
- The auscultation locations are focused on listening to the valves, though the names of the locations do not necessarily correlate with where the same valve is heard best.
- Aortic: second intercostal space, right sternal border (2ICS-RSB)
- Pulmonic: second intercostal space, left sternal border (2ICS-LSB)
- Tricuspid: left lower sternal border (about the fifth intercostal space; LLSB)
- Mitral: cardiac apex at the fifth intercostal space, mid-clavicular line (5ICS-MCL)
- Erb's point: third intercostal space, left sternal border (3ICS-LSB)
- Location of best pulmonic / aortic valve auscultation

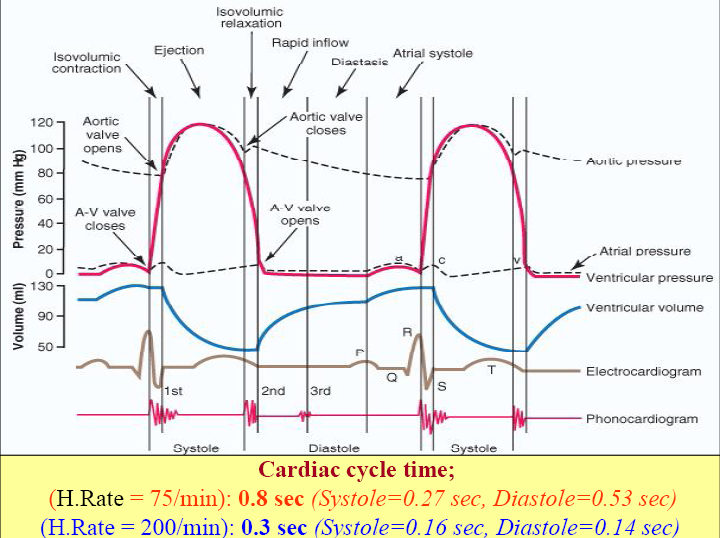
[edit] Describe the cardiac cycle and be able to clinically correlate the cycle to a patient’s cardiac exam
- There are four heart sounds: S1, S2, S3, S4
- S1 is the closure of the AV valves: mitrial (left, systemic side) and tricuspid (right, pulmonary side)
- S2 is the closure of the semilunar valves: aortic (left, systemic side) and pulmonary (right, pulmonary side)
- S1 and S2 are normally audible in all individuals.
- S3 and S4 are normal in children and young adults but indicate pathology in adults.
- The presence of S3 or S4 creates a gallop sound and thus they are called gallop sounds.
- S3 occurs at the end of rapid ventricular filling.
- S3--when audible--indicates volume overload.
- Causes of volume overload may include CHF or valve lesions causing regurgitation.
- S3 has a specificity of 90%.
- NB: is is normal to hear S3 in children and youth.
- S4 occurs at the end of diastole.
- S4 can be simulated by speaking the word "middle". S4 is the "ddle" of "middle" where the "mi" is S1 (closing of AV valves).
- NB: S4 is normal in children and young adults.
- S4 in a pt older than 40 is indicative of a noncompliant or stiff ventricle.
- Pressure overload as in CHD is the cause of a noncompliant ventricle.
- Physiologic split of S2 with accompanied sinus arrythmia:
- S2 is often split, especially upon inspiration.
- During inspiration, the intrathoracic pressure is lower causing more blood from the SVC and IVC to enter the right atrium / ventricle.
- Increased right heart filling results in a longer duration of systole and therefore a later closure of the pulmonic valve.
- Thus P2 (the pulmonic component of S2--that is, the closing of the pulmonic valve) occurs later than A2 (the aortic component of S2--that is, the closing of the aortic valve).
- Initially, the return of blood from the pulmonic bed to the left heart will be relatively decreased so the left heart reflex induces sinus arrythmia.
- Sinus arrythmia is an increased heart rate after respiration and is a misnomer because it is not a true arrythmia.
- http://howmed.net/wp-content/uploads/2010/09/cardiac-cycle.bmp


[edit] Recognize the main symptoms of cardiac disease and how these symptoms can identify disease
- The main symptoms of cardiac disease are: chest pain, palpitations, dyspnea, syncope, fatigue, dependent edema, hemoptysis, and cyanosis.
[edit] Chest pain
- Not specific to the heart yet the most important.
- Angina pectoris: pain resulting from an imbalance of myocardia perfusion and myocardial functional demand.
- Classically presents as the pathognomonic Levine's sign: clutching fist over sternum with flexion at the hips.
| Descriptor | Angina | Non Angina |
|---|---|---|
| Location | Retrosternal, diffuse | Left inframammary, localized |
| Radiation | Left arm, jaw, back | Right arm |
| Character | Aching, dull, pressing, squeezing, viselike | Sharp, shooting, cutting |
| Intensity | Mild, severe | Excruciating |
| Duration | Minutes | Seconds, hours, days |
| Precipitation | Effort, emotion, eating, cold | Respiration, posture, motion |
| Relief | Rest, Nitroglycerin | Nonspecific |
- Common causes of chest pain include: CAD, aortic valvular disease, pulmonary hypertension, mitral valve prolapse, pericarditis, idopathic hypertrophic subaortic stenosis, dissection of the aorta, pulmonary embolism, penumonia, pleuritis, pneumothorax, costochondritis, arthritis, muscular spasm, bone tumor, herpes zoster, ulcer disease, bowel disease, hiatal hernia, pancreatitis, cholecystitis, anxiety, depression.
[edit] Palpitations
- Palpitations are not necessarily a sign of disease.
- Palpitations are often reported upon the occurrence of "forceful contraction" which result from increased stroke volume.
- Consider: primary cardiovascular issues, thyrotoxicosis, hypoglycemia, fever, anemia, pheochromocytoma, and anxiety.
- Consider: caffeine, tobacco, other drugs
- Common causes: atrial premature beats, nodal premature beats, ventricular premature beats, paroxysmal supraventricular tachycardia, atrial flutter, atrial fibrillation, multifocal atrial tachycardia, ventricular tachycardia, heart block, sinus arrest, bronchodilators, digitalis, antidepressants, smoking, caffeine, thyrotoxicosis
[edit] Dyspnea
- Paroxysmal nocturnal dyspnea occurs when the pt is supine (usually sleeping at night).
- Supine position increases blood volume in the thorax and therefore the work of the right heart, resulting in heart failure.
- Orthopnea may be reported: the need to sleep propped up on many pillows.
- Look for pitting edema in the legs as another indicator of heart failure.
- Dyspnea on exertion (DOE): occurs via pulmonary disease or chronic congestive heart failure
- Trepopnea: when a pt has less dyspnea when lying on the right or left side.
- General causes of dyspnea include: left ventricular failure, mitral stenosis, obstructive lung disease, asthma, restrictive lung disease, pulmonary embolism, pulmonary hypertension, anxiety, decreased oxygen pressure, and decreased oxygen carrying capacity.
[edit] Syncope
- Syncope is defined as loss of consciousness AND loss of postural tone.
- Orthostatic hypertension can lead to syncope.
- Micturition syncope occurs in older men (usually) who have to urinate during the night and (because they have just moved from supine to standing) experience syncope.
- Vasovagal syncope occurs because of a sudden fall in systemic vascular resistance without a compensatory increase in cardiac output (because of increased vagal--parasympathetic--signal).
- Usually accompanied by presyncopous s/s: pallor, nausea, weakness, blurred vision, light headedness, perspiration, yawning, diaphoresis, hyperventilation, epigastric discomfort (sinking feeling).
- Carotid sinus syncope occurs because of an hypersensitive carotid sinus (or excessive stimulation of the carotid sinus) which leads to inappropriate baroreceptor signaling that leads to hypotension and a risk of syncope.
- The reflex can cause bradycardia (slowing the heart rate, decreasing perfusion of the brain, and syncope) or vasodepression (decreased vasoconstriction, decreased perfusion, and syncope).
- Post-tussive syncope is when coughing increases the thorasic pressure (usually in pts with chronic obstructive disease) and thus activates the carotid sinus reflex and induces syncope.
[edit] Fatigue
- Most common causes of fatigue are anxiety and depression.
- Fatigue has poor specificity for cardiac issues.
[edit] Dependent Edema
- Dependent edema means that it is a function including gravity; that is, dependent edema is edema that is affected by gravity.
- Classically, dependent edema is seen in the lower limbs and it best in the morning after having been supine for hours and is worse at the end of the day when the pt has been upright and gravity has moved the fluid to the legs.
- Symmetrical swelling indicates a systemic cardio-pulmonary issue as opposed to an infectious agent.
- Cardiac causes of edema are usually preceded by dyspnea.
[edit] Hemoptysis
- Hemoptysis is the coughing up of blood.
- Mitral stenosis is an important cuase of hemoptysis.
- More in chapter 13.
[edit] Cyanosis
- Differential cyanosis is when cyanosis is seen only in the lower extrimities.
- Differential cyanosis is related to a right-to-left shunt (usually through a patent ductus arteriosus).
- Right-to-left shunt at the ductus arteriosus usually results from pulmonary hypertension.
- Cyanosis occurs only in the lower extremities because blood from the pulmonary artery (deoxygenated) mixes below the carotid / subclavian (which would take the blood to the head / arm).
[edit] Interpret the symptoms of cardiac disease from a clinical scenario..........
[edit] Apply the components of the physical exam of the heart to a patient
[edit] Inspection
- Xanthomata are deposits of stony-hard, slightly yellowish masses found on extensor tendons of fingers.
- Pathognomonic for hypercholesterolemia.
- Think plantar and tendons of the soles of the feet.
- Primary biliary cirrhosis can lead to extremely high levels of cholesterol and therefore xanthomas.
- Antimitochondrial antibodies is found in 90% of patients with primary biliary cirrhosis.
- Eruptive xanthomata are seen in hyperlipidemia and are characterized as being on the chest, buttocks, abdomen, back, face, and arms.
- These are elevations of serum triglycerides to levels near 1500 mg / dL.
- Erythema that is disc shaped with raised edges is called erythema marginatum and can indicate acute rheumatic fever.
- Osler's nodes are painful lesions at the tufts of the finger and toes that indicate infective endocarditis.
- Splinter hemorrhages have a low specificity; they can indicate trauma, poor oxygenation, or endocarditis.
- Supravascular aortic stenosis can be characterized by wide set eyes, strabismus, low-set ears, upturned nose, and hypoplasia of the mandible.
- Pulmonic stenosis can be indicated by moon facies and widely spaced eyes.
- Hypothyroidism commonly manifests as puffy eyelids, stoic expression, and loss of the outer third of the eye brows.
- Lichtstein's sign is a lateral earlobe crease that may indicate CHD in pts over 50 yo.
- High cholesterol and / or protein levels show up in the eye as xanthelasma, though this is less specific than xanthomas.
- Arcus senilus in pts younger than 40 should raise suspicion regarding hypercholesterolemia.
- Sarcoidosis leads to opacity of the cornea.
- Marfan syndrome often produces lens dislocation.
- A high palatal arch in the mouth may indicate congenital heart disorders like mitral valve prolapse.
- Petechia on the palate may suggest infective endocarditis.
- Webbing of the neck may indicate Turner syndrome (single X, girls) which has increased risk for coarctation of the aorta.
- Webbing may also be associated with Noonan's syndrome which is associated with pulmonic stenosis.
- External chest deformations like pectus excavatum or pectus carnatum may indicate underlying cardiac development issues.
- As in Marfan's syndrome.
- An extra finger, toe, or phalanx is sometimes seen with atrial septal defects.
- Long, slender fingers are associated with Marfan's syndrome which is associated with cardiac issues.



[edit] Blood Pressure Assessment
- When using a sphygmomanometer, one is measuring the appearance and disappearance of the Korotkoff sounds.
- The point of hearing the first sounds indicates the systolic pressure.
- The point of hearing only muffled sounds indicates the top pressure range of the diastolic pressure.
- When the point of muffled and the point of not-even-muffled is more than 10mgHg apart, the point of only muffled sounds is more accurate.
- The point of hearing not even muffled sounds indicates the lower pressure range of the diastolic pressure.
- Blood pressure should be recorded at the nearest 5mmHg because all sphygmomanometers have a +/- 3mmHg accuracy.
- Ausculatatory gap occurs in hypertension; it is the disappearance of the Korotkoff sounds and then reappearance before finally disappearing at the diastolic pressure interval.
- Retake the blood pressure at the end of the examination when the pt may be more relaxed.
- Orthostatic hypotension is a drop of blood pressure by more than 20mmHg upon standing (and is associated with dizziness or syncope).
- Supravalvular aortic stenosis is indicated by hypertension in the right arm and hypotension in the left arm.
- Coarctation of the aorta is indicated by leg blood pressures that are lower than those of the arms.
- Recall that a blood pressure can be taken at the thigh / knee (with auscultation at the popliteal artery in the popliteal fossa) or at the leg / ankle (with auscultation at the dorsalis pedis or posterior tibial arteries).
- Check for infant femoral pulse to screen for coarctation of the aorta.
- Cardiac tamponade is indicated by paradoxical pulse: a difference in systolic pressure greater than 10mmHg when heard only at rest and when heard only upon inspiration.
- To test: while taking decreasing the pressure of the sphygmomanometer with the pt breathing normally, note the pressure at which Korotkoff sounds are heard only upon expiration and then the pressure at which sounds are heard only upon inspiration.
- Paradoxical pulse can also be heard in pericardial effusions, constrictive pericarditis, and increased ventilatory effort (asthma, emphysema).
| Observation | Example | Associated disease state |
|---|---|---|
[edit] Arteriole Pulse
[edit] Jugular Venous Pulse
[edit] Percussion
[edit] Palpation
[edit] Ausculation
[edit] Clinically correlate the symptoms and physical exam findings pertaining to the heart
[edit] Give a diagnosis and/or differential diagnosis based on symptoms and/or physical exam findings of the heart
[edit] Describe findings from the history and physical exam in the written history and oral case presentation
[edit] Chapter 16: Breast
- Pages 455-476
- Differentiate the clinical significance of a lump that enlarges during the premenstrual and menstrual stages of the cycle and the breast lump which does not change during the menstrual cycle.
- A breast lump that enlarges during premenstrual / menstrual stages is likely physiological nodularity
- Describe and identify the changes of the skin and nipple which are strongly suggestive of neoplasm.
- Characteristics associated with neoplastics changes of the breast include nipple discharge, nipple inversion, skin changes overlying a mass.
- Describe the different types of nipple discharge. Differentiate and identify the different types of nipple discharge and their clinical significance.
- Types of nipple discharge include: serous (thin, watery, yellowish), bloody, and milky.
- NB: both serous and bloody types of discharge can be associated with malignancy so the the presence of discharge is more important than the type of discharge.
- Serous discharge commonly results from intraductal papilloma in one of the large subareolar ducts, with oral contraceptive use, or with carcinomas.
- Bloody discharge commonly results from intraductal papilloma (as with serous discharge), too.
- Describe the components of the physical examination of the breast and the proper positioning of the patient for each component.
- The components of the breast PE include inspection (seated; hands on hips; hands pulling apart a shoulder level; hands above head; leaninig forward), axillary examination (pt seated; arm held up away from axilla), and paplation (pt lying; hand above head; shoulder on table; potentially leaned toward opposite side to distribute breast over chest wall).
- Describe the following changes of the breast: erythema, edema, and dimpling. Identify and describe the differential diagnosis for each of the above physical findings.
- Erythema: Erythema is an important symptom of breast carcinoma.
- Edema: Edema is characterized by the prominent pores and is an important sign of malignancy called peau d'orange. (Lymphatics are clogged by emboli of tumor tissue.)
- Dimpling: The presence of dimpling warrants further investigation.
- Describe the proper physical exam technique for axillary examination. Describe and name which lymph node regions that should be palpated on physical examination.
- With the pt seated and arm abducted away from the body (lay arm over examiner's shoulder), pectoral muscle relaxed, make dime-size circles with the pads of the fingers (without losing contact with the skin), working superiorly. Palpate the anterior and posterior aspects of the axilla. Adduct the arm as one moves superiorly to allow for deep, superior palpation.
- Palpate the supraclavicular nodes and infraclavicular nodes.
- Freely moving nodes (3-5 mm) are common and usually due only to lymphadenopathy.
- Describe the characteristics which should be used to describe a breast mass which is found on physical examination.
- Skin condition, symmetry, dimpling, masses, discharge, and lymphadenopathy should all be addressed.
- Skin should be described in color and texture.
- Discharge should be characterized by consistency and color.
- Dimpling should be described as location on the clock and from the nipple.
- Masses should be described in size and texture.
- Nodes should be described in motility and texture.
- Based on a clinical description, differentiate between cystic disease, a benign adenoma, and a malignant tumor.
| Trait | Cystic Disease | Benign Adenoma | Malignant Tumor |
|---|---|---|---|
| Pt Age | 25-60 | 10-55 | 25-85 |
| # of masses | 1+ | 1 | 1 |
| Shape | Round | Round | Irregular |
| Consistency | Elastic, soft, hard | Firm | Stony hard |
| Delimitation | Well delimited | Well delimited | Poorly delimited |
| Mobility | Mobile | Mobile | Fixed |
| Tenderness | Tender | None | None |
| Dimpling | None | None | Dimpled |
- Note that malignant tumor traits have low sensitivity:
- Mobility fixed: 90% spec, 40% sens
- Poorly delimited: 90% spec, 60% sens
- Consistency hard: 90% spec, 62% sens
- 50% of fixed masses are cancerous; 60% of fixed, irregular masses are cancerous;
- Classic description of a benign mass is mobile, well circumscribed, soft or cystic.
- Classic description of a cystic mass is multiple, tender, mobile, elastic (soft or firm), well circumscribed.
[edit] Chapter 15: Peripheral Vascular System
- Pages 438-454
- Define and describe the components for the physical examination of the peripheral vascular system.
- Unlikely to be a test question; just watch the video.
- Differentiate ulcers caused by arterial insufficiency and venous insufficiency.
- Arterial insufficiency ulcers: cool / pale limb with painful, rapid onset, punched out, crusted lesions on the heels and toes.
- Venous insufficiency ulcer: warm / erythematous limb with painless (early at least), insidious, diffuse, reddened, thickened lesions superior to the medial maleolus.
- Define and differentiate intermittent claudication and pseudoclaudication.
- Intermittent claudication is unilateral (usually) pain in the lower limb upon exertion and worsened by cold temperatures or elevation.
- Claudication pain is usually in the calf, arch of the foot, thighs, hips, or buttocks.
- Pseudocladucation is bilateral numbness or pain in the legs that results from musculoskeletal pathology in the lumbar area.
- Intermittent claudication is unilateral (usually) pain in the lower limb upon exertion and worsened by cold temperatures or elevation.
- Differentiate skin changes caused by arterial insufficiency and venous insufficiency.
- Arterial insufficiency is marked by paleness and coolness (no blood / warmth gets there).
- Venous insufficiency is marked by warmth, erythema, and excoriations (from scratching at pruritis).
- Identify important risk factors for the development of thrombus formation.
- Anything that causes or increases blood stasis increase the risk of thrombus formation.
- Risk factors for thrombus formation include: bed rest, congestive heart failure, obesity, pregnancy, extended airplane travel, and oral contraceptives.
- Recognize the symptoms of emboli affecting various organ systems.
- Pulmonary embolic symptoms: shortness of breath (think pulmonic arteries)
- Abdominal embolic symptoms: pain (think splenic, intestinal, and renal arteries)
- Neuro embolic symptoms: syncope, confusion, coma etc. (think carotid and vertebrobasilar arteries)
- Peripheral embolic symptoms: pain and paresthesias (think brachial artery, etc.)
- Clinically correlate abnormal findings when found on the examination of the arterial system. The student should be able to correlate and interpret the physical finding with the following disease processes:
- S&S of abdominal aortic aneurysm: a laterally expansive pulsatile mass may be palpated, abdominal bruit, femoral bruit, femoral pulse deficit, pain (in the back and abdomen, upon rupture).
- Be careful not to interpret a normal aorta in the thin pt as an aneurysm.
- Auscultate for AAA 2 inches above umbilicus, at midline.
- Abdominal bruits heard only during systole are usually not pathologic.
- S&S of renal artery stenosis: auscultated bruit (99% specificity, 39% sensitivity)
- A renal bruit is considered combined systolic-diastolic and is found 2 inches above and 2 inches lateral to the umbilicus.
- S&S of coarctation of the aorta: delayed femoral pulse as compared to radial pulse.
- Recall that the femoral pulse should arrive just before or at the same time as the radial pulse in normal physiology and anatomy.
- Be especially suspicious of coarctation of the aorta in hypertensive individuals.
- S&S of obstructive aortoiliofemoral disease: delayed / diminished comparison of femoral pulses, femoral bruit.
- S&S of atherosclerosis of the carotid artery: carotid bruit may be auscultated (with pt in supine position with head on pillow), carotid murmur may be auscultated (can also be a loud murmur from the heart)
- S&S of peripheral vascular disease: decreased pulses, excessive / prolonged pallor, poor reperfusion, incompetent saphenous vein.
- Recall, also, the five p's: pain, pallor, paresthesia, paralysis, and pulselessness.
- S&S of abdominal aortic aneurysm: a laterally expansive pulsatile mass may be palpated, abdominal bruit, femoral bruit, femoral pulse deficit, pain (in the back and abdomen, upon rupture).
- Define and differentiate generalized lymphadenopathy, localized lymphadenopathy, lymphangitis, and lymphedema.
- Generalized lymphadenopathy: the presence of palpable lymph nodes in three or more lymph node chains.
- Generalized lymphadenopathy suggests a systemic diagnosis like lymphoma, leukemia, collagen vascular disorders, and systemic bacterial / viral / protozoal infections.
- Localized lymphadenopathy: the presence of palpable lymph nodes in less than three lymph node chains.
- Localized lymphadenopathy suggests a localized infection or neoplasm.
- Lymphangitis: lymphatic spread of infection or neoplasm manifesting thin, red streaks on the skin.
- Recall the fungus Sporothrix schenckii which is common is gardners and florists that get pricked by rose thorns. It works its way up the lymphatics of the arm, leaving a string of ulcers or nodules.
- Lymphedema: resulting from obstruction of lymphatic drainage, this type of edema is usually firm and non-pitting as compared to vascular edema which is usually pitting.
- Generalized lymphadenopathy: the presence of palpable lymph nodes in three or more lymph node chains.
- Define and appropriately apply the Allen test on a patient. The student should be able to interpret the findings of this test.
- The Allen test detects arterial insufficiency in the upper extremities, specifically the ulnar and radial arteries.
- The test is based on expected, normal refill when either the ulnar or radial artery are compressed and the hand is emptied of blood (pt makes a fist).
- If, upon opening the fisted hand, there is delay of refilling, the opposing artery may be insufficiency. (That is, if you compress the radial artery, have the pt make a fist, have them open it, and observe poor refilling, then the ulnar artery may be insufficient).
- The Allen test!
[edit] Chapter 22: Integrating the exam
- 696-706
[edit] Chapter 1 (Lange): I Have a Patient with a Problem: How do I figure out the possible causes?
- Pages 1-9
- Define the steps in the diagnostic process.
- Define sensitivity, specificity and likelihood ratio.
- Understand how true negatives, false negatives, false positives and true positives are determined.
[edit] Chapter 8 (Lange): Chest Pain
- Pages 130-148
- Know the differential diagnosis of chest pain by anatomical organization.
- Know the key factors in the history and on physical examination and initial diagnostic evaluation that accompany each of the following diagnoses:
- Stable Angina
- GERD
- Myocardial Infarction
- Unstable Angina
- Aortic Dissection
- Pleural Effusion
- Acute Pericarditis

{kind=link}